
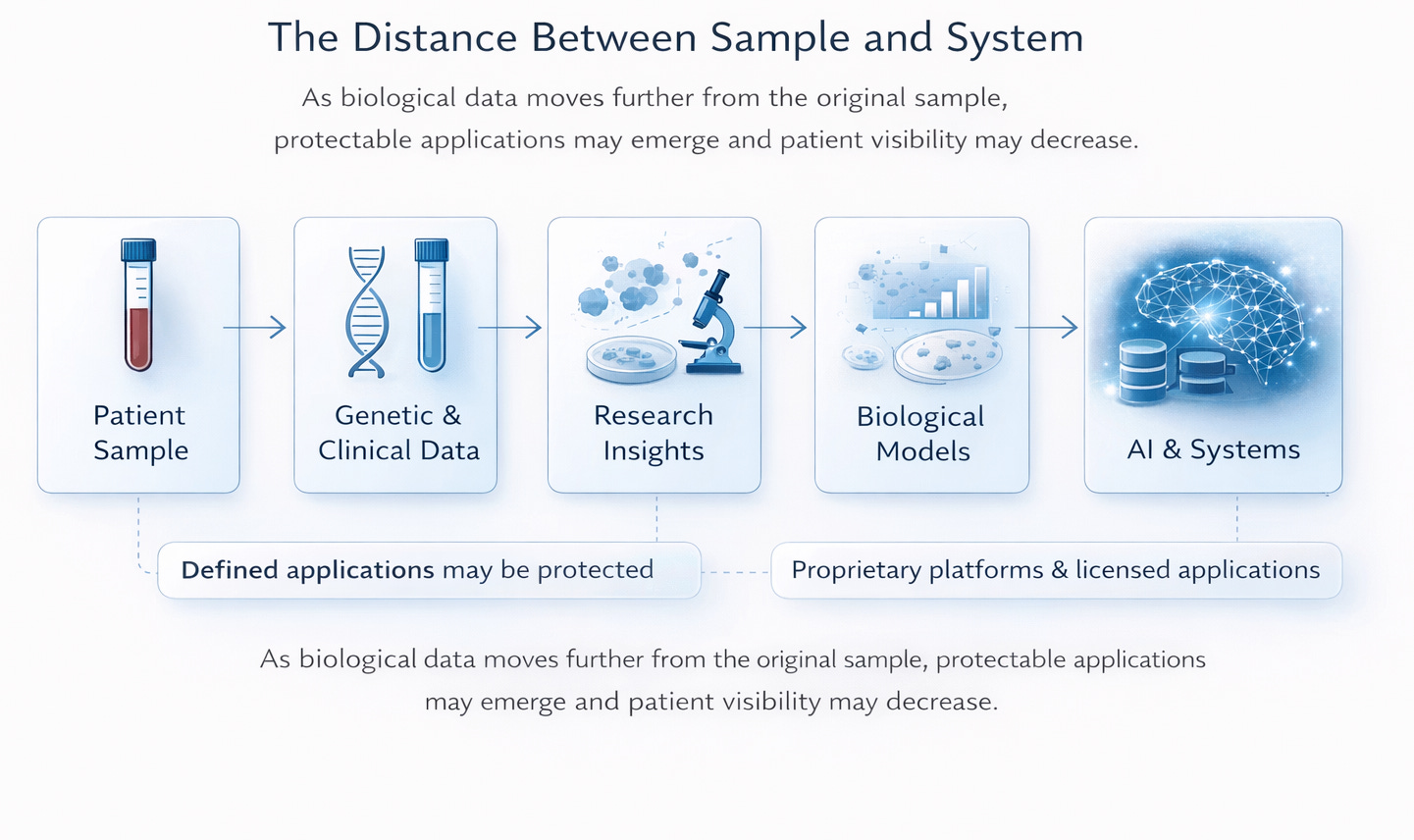
From Sample to System
Entering a New Structural Reality


I have been collecting a lot of my own data.
Some of it comes from standard clinical testing, some from genomic analysis, and some reaches a level of biological detail that, until recently, was largely confined to research settings. In a few instances, the information I’m looking at is still new even to my own doctor.
I track it because I want to understand what’s happening inside my body. I compare results over time. I share parts of it for research because I believe progress in rare disease has always depended on patients being willing to contribute.
Lately, as I’ve been sharing more of it, I find myself thinking less about security and privacy and more about where it goes and how it’s being used.
A blood draw used to generate lab values, and that was usually the end of it. Now that same sample can generate genomic information, patterns of gene activity, immune system signals, and sometimes laboratory models that continue long after the appointment itself. Those data points do not stay in one place. They are combined with thousands of others to help researchers understand how a disease works, identify treatment targets, and build computational systems that learn from aggregated information.
I understand how that process works because I live in this space. Intellectual property is part of how therapies eventually move from discovery to market, and protection is built into that system for a reason.
But when the data in question is my own, it feels different.
My blood and my cells are not patentable just because they are mine. But insight drawn from them can be developed into something concrete, such as a therapy, a diagnostic platform, or a specific technical method. Those applications can later be protected through patents or licensing. They can shape investment, influence access, and structure the direction of research long after the original sample was taken.
Meanwhile, I am still here living with the condition that made that data possible in the first place.
That is where the nervousness comes in.
I am passionate about this work and genuinely excited by what is possible. But I also feel nervous, because I know how much can shift once data moves beyond the individual.
When it is your body, the stakes feel different. Misinterpretation is not abstract. A rare disease patient can become an outlier in a model that lacks context. Decisions made at scale by insurers, employers, or institutions do not always reflect lived reality. And while platforms can grow from aggregated data, the people who contributed that data often remain economically and structurally constrained.
For patients like me, those risks are not hypothetical. They are part of what we have to consider every time we decide whether to share.
Because I move between clinical care, research conversations, and industry settings, I see how the meaning of the same contribution shifts. What feels deeply personal in one room becomes technical in another. As the work scales, it becomes easier to talk about datasets and systems than about the people who made them possible.
Intellectual property plays a real role in bringing therapies to market. My concern is not that it exists. It is that the frameworks governing participation were built at a time when patients did not hold this level of biological insight themselves.
We are entering a moment where patients can access and generate data at a depth once reserved for research laboratories. The governance structures around participation, including privacy protections, consent language, and institutional review, were not designed with that reality fully in mind.
They protect entry into research. They do not always account for what happens as value accumulates downstream.
In rare disease especially, where patient populations are small, contribution is not abstract. A handful of families may make foundational discoveries possible. Development may follow. Investment may follow. Protected applications may emerge. Yet the patients whose biology made that possible may still be navigating insurance limits, federal program income thresholds, and the daily realities of living with a chronic condition.
That imbalance is not always intentional. It is structural.
As I continue to collect and share my own data, I am trying to hold that structural shift in view. Not only the immediate study or the next dataset, but the longer arc from sample to system.
A tube of blood can now move far beyond the clinic. It can become part of a dataset, a laboratory model, an engineered therapy, or an algorithm that persists over time. I know where my data begins.
What I’m still trying to understand is how far it travels, and whether the systems built from it are ready for patients who are no longer just subjects of research, but holders of research-level insight themselves.